- Available 24X7 for Emergencies
- For meeting on any day from Monday to Saturday…Kindly call on 9924148081 one day prior to fix up the time of meeting for next day
2D & 3D EP Study+RFA
2D & 3D EP Study+RFA
What is an Electrophysiological Study (EPS)?
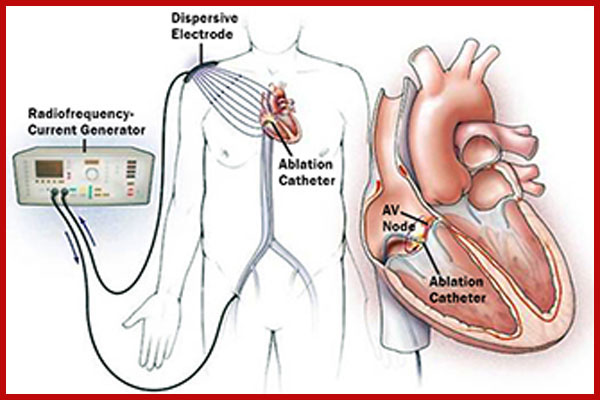
An electrophysiological study is a test that looks at the electrical activity of the heart, allowing the doctor to diagnose and analyse fast or abnormal heart rhythms. It is able to give more detailed information than an external electrocardiogram (ECG). It involves a fine tube called a catheter being inserted into the heart via a blood vessel (vein or artery) in the groin. The end of this catheter has a special electrode tip which stimulates the heart and records the electrical activity allowing the doctor to identify where any abnormalities may be coming from.
3D electroanatomical navigation mapping systems can display the position of catheters in real time on a computer screen, and reconstruct the detailed 3D surface anatomy of a given cardiac chamber, while tagging this reconstructed endocardial or epicardial surface geometry–appearing as a shell in the virtual 3D space.
What is a Radio Frequency Ablation (RFA)?
Radiofrequency ablation is a treatment that aims to control or correct an abnormal heart rhythm. It is carried out in the same way as an electrophysiological study (EPS) by inserting catheters into heart via the groin. Radiofrequency energy (heat) is then used to destroy the small area in the heart where the abnormal electrical activity is coming from. This can be done at the same time as the EPS or on a separate occasion.
Why do I need an EPS and RFA?
You will usually have been experiencing symptoms of palpitations or a racing heart beat which can be quite distressing at times for some people. This is because sometimes, the electrical conduction system in the heart travels in a different direction due to extra electrical connections known as ‘pathways’, or due to extra electrical cells within the heart. Often these pathways are present at birth, but may only start to cause symptoms in adulthood. When the heart has an extra beat (an ectopic beat), it can travel up the pathway and travel down the normal conduction system. If this continues, palpitations can start. This means that the heart suddenly starts to race, causing an awareness of a fast heartbeat.
If the abnormal heart rhythm is arising from the upper chambers of the heart, this is known as SVT, or supraventricular tachycardia. This type of heart rhythm disturbance is not life threatening, but can cause unpleasant symptoms and interfere with your quality of life. If the abnormal heart rhythm comes from the lower pumping chambers of the heart (the ventricles) it is called VT, ventricular tachycardia, which can be dangerous, particularly if it is associated with fainting.*
Can there be any complications or risks?
These procedures do carry a small amount of risk. Your doctor will explain this to you before you give your consent to have the procedure done. Bruising in the groin area is the most common complication and is usually nothing to worry about.
With RFA there is a small risk of damage to the heart’s normal electrical pathways. If this happens there is a small risk that you may require a pacemaker. You will have many opportunities to discuss any questions or concerns with the nurses and doctors caring for you before undergoing the test.
When it is time for your procedure a nurse from the Cath Lab will come to the ward to collect you. They will go through the safety checklist again before accompanying you into the Lab.
Once inside you will be helped onto the X-ray table and asked to lie flat on your back with one pillow for your head. The skin in your groin area will be cleaned with a cold antiseptic solution then your body will be covered with a sterile theatre towel.
A sheath (similar to the cannula) is then inserted into the blood vessel in your groin and thin flexible tubes (called catheters) are inserted through it and using an X-ray machine are gently guided into the correct position inside of your heart. You may feel an unusual sensation or discomfort in your chest as the catheters are inserted but this should not be painful.
Once the wires are positioned within the heart, extra beats are delivered using an external pacemaker, which may bring on your palpitations. This is necessary to see the area of the heart where the abnormal rhythm is coming from. It is possible to put the heart back into normal rhythm within a few seconds, by delivering some extra beats, so whilst you may feel a little strange the procedure is completely under the control of the doctor and their team.
Once the abnormality has been found and if it is felt to be necessary, the doctor performing the procedure will then begin to ablate the pathway or area of extra electrical cells. This is done by delivering a form of energy (radio frequency) down the catheter wire to the target area within the heart. The procedure can take up to 4 hours depending on the nature of the problem.*
What will happen afterwards?
When the procedure is over, the catheters and the sheath are removed from the groin area. A doctor or nurse will press firmly on the area for several minutes to stop any bleeding. When you are back on the ward you will be attached to a cardiac monitor and need to lay flat in bed for 1 hour (after the sheaths are removed) and then complete a further 1 hour of bedrest. Your nurse will also take your blood pressure every so often and keep checking your wound to make sure it is not bleeding and there is no unusual swelling. You will be able to get out of bed and mobilise after the period of bedrest if the nurse is happy with your wound and your blood pressure. If you are well you will be allowed home approximately 4 hours after your return to the ward.*






